December 1 is World AIDS Day. HIV is still a global pandemic with a staggering 1.3 million new cases in 2023—that’s 1 new transmission every 30 seconds. In 2022, Canada saw a 25 percent increase—the largest leap in cases in over a decade.
WEAR A RED RIBBON & SHOW YOUR SUPPORT FOR CANADIANS LIVING WITH HIV.
WEAR A RED RIBBON & SHOW YOUR SUPPORT FOR CANADIANS LIVING WITH HIV.
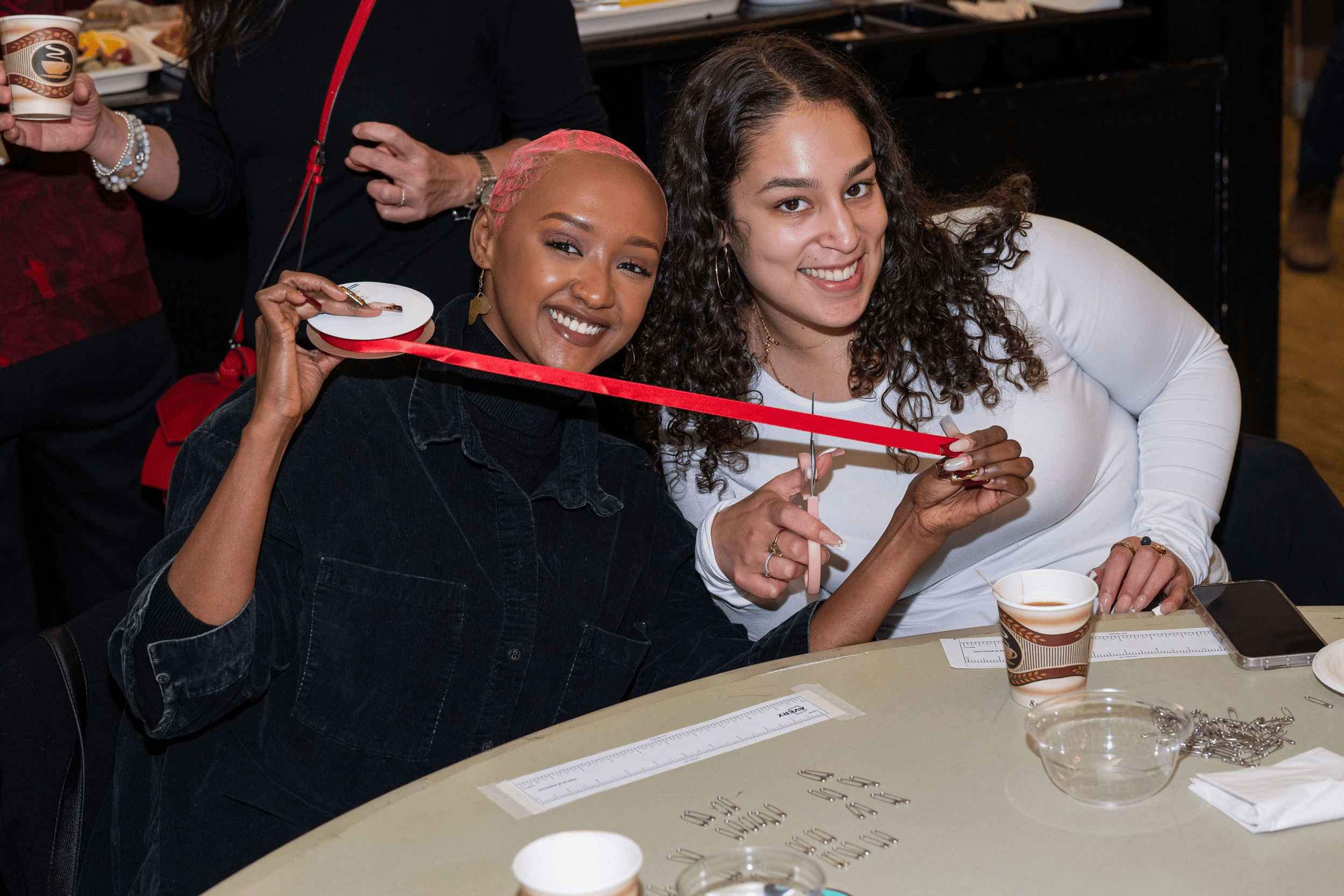
Learn how to make a wearable red awareness ribbon with HIV advocate Muluba Habanyama. All you need is red ribbon and a small safety pin!
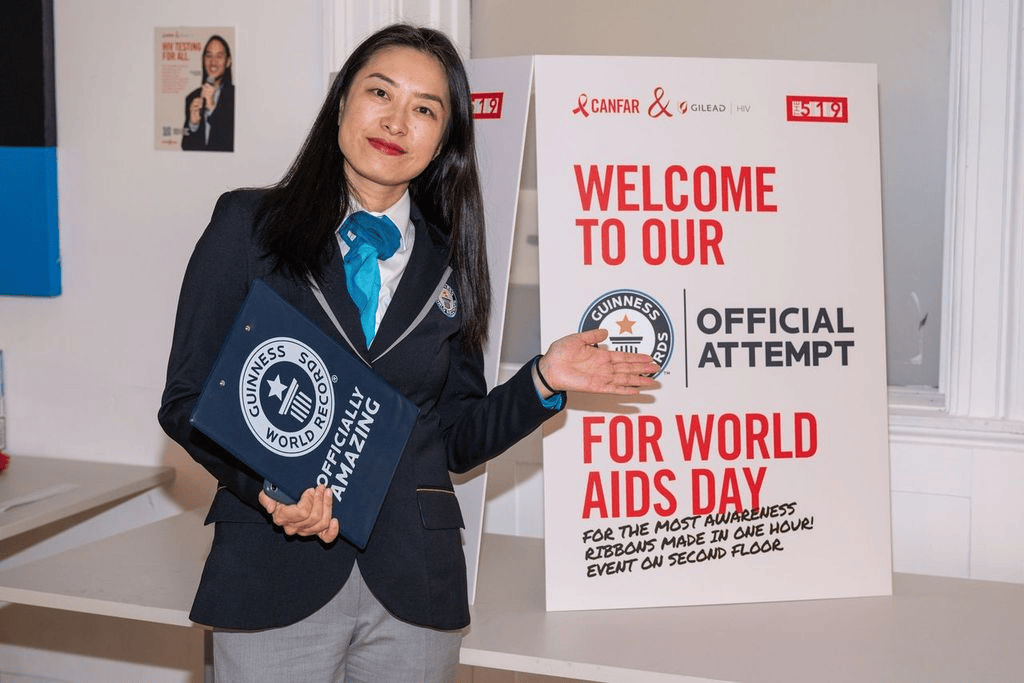
it’s official: we broke the world record for the most awareness ribbons made in one hour in toronto. then, we set the world record for the largest awareness ribbon mosaic in ottawa. check out the galleries and share on social media using #myredribbon!
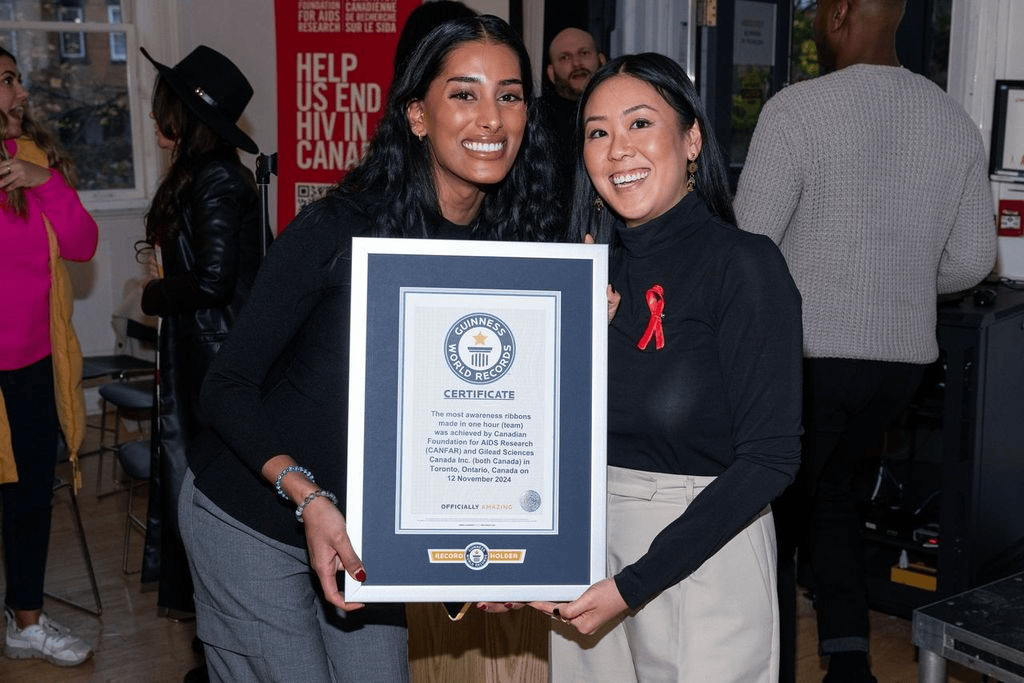
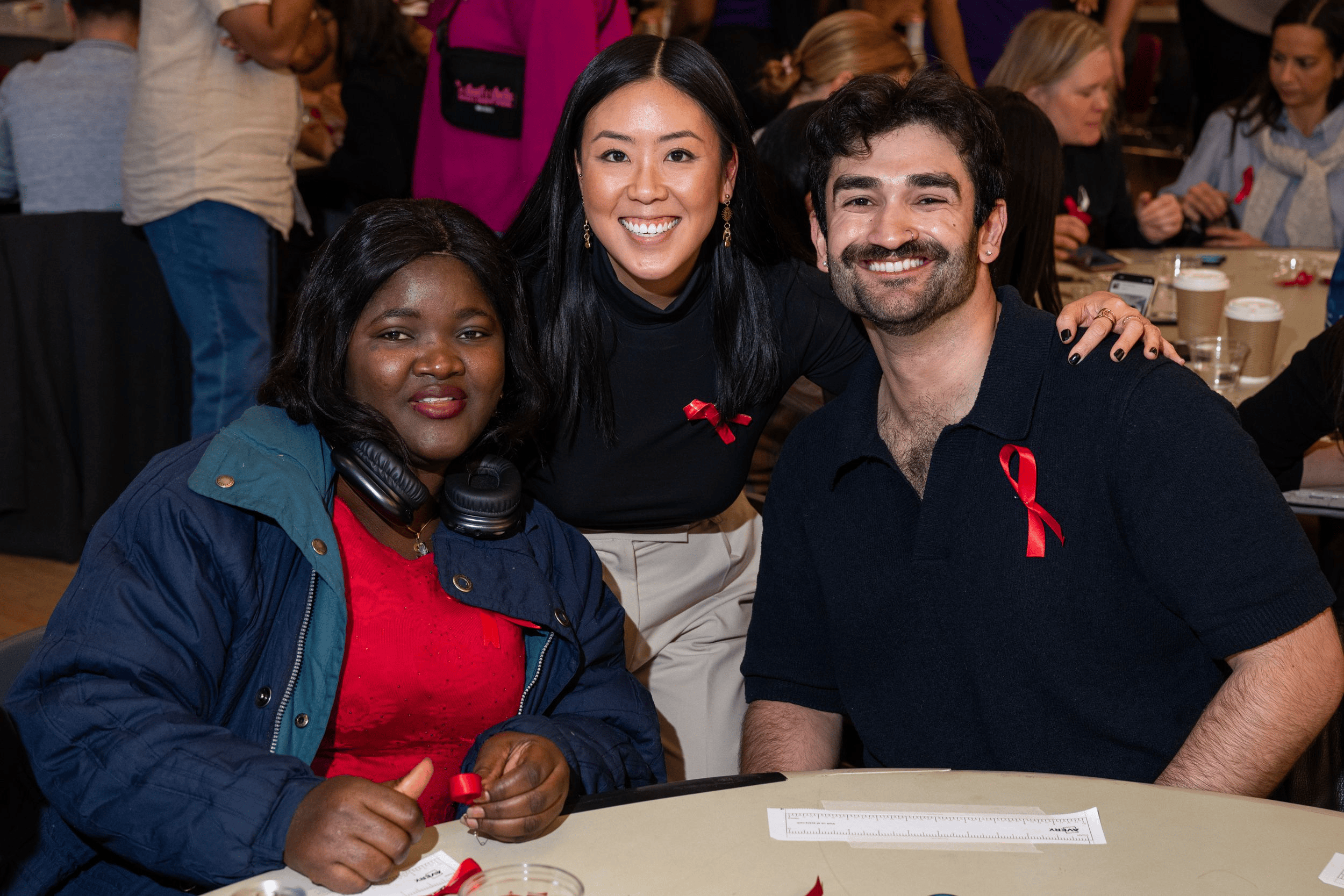
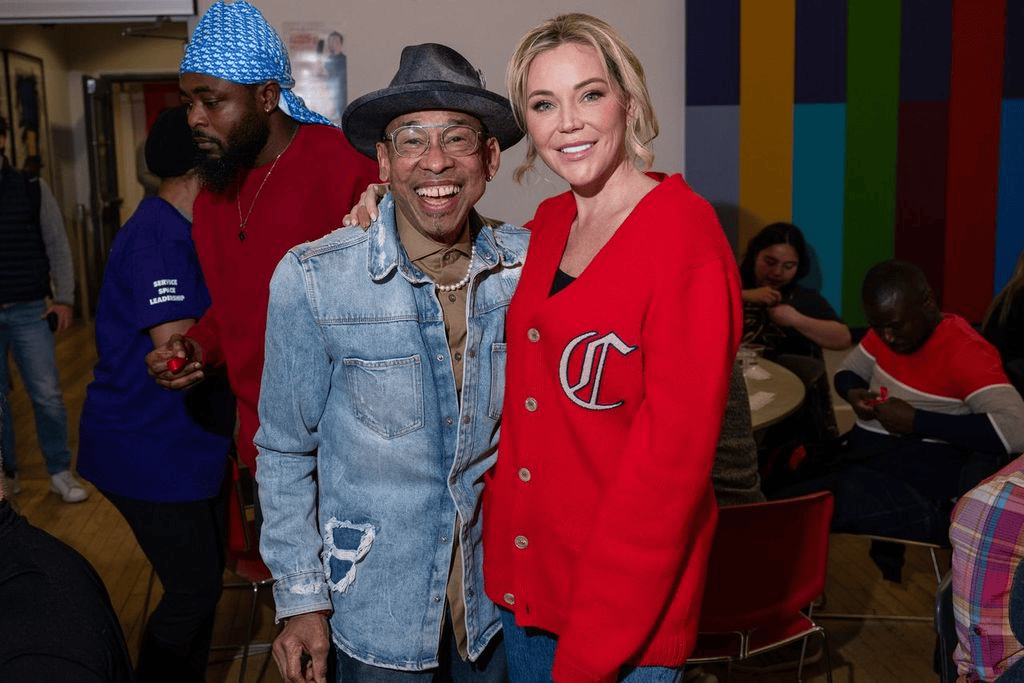
Tues., Nov. 12: at the 519 Community Centre (Toronto)
We broke the Guinness World Records Title for the most awareness ribbons made in one hour! The previous record was 5,471. Our community came together and made 11,255 ribbons. Special shout-out to longtime HIV survivor Billy Newton-Davis for his incredible role as our expert judge.
Download and share the gallery using #myredribbon. Please credit @matt_tibbo_photography and @ryanemberley, and tag @canfar1987, @the519, @gileadsciences, and @guinnessworldrecords.
We set the Guinness World Records Title for the largest awareness ribbon mosaic made of awareness ribbons! This new record needed a surface area of 25 square meters, and we measured in at 29.706 meters squared!
Download and share the gallery using #myredribbon. Please credit @szemingwu, and tag @canfar1987, @centretownbia, @gileadsciences and @guinnessworldrecords.
DO YOU KNOW HOW TO BE AN ALLY THIS WORLD AIDS DAY?
DO YOU KNOW HOW TO BE AN ALLY THIS WORLD AIDS DAY?
Wear a red ribbon. Use #myredribbon on social media. Donate to your local AIDS-service organization. Educate yourself, your friends & family about the realities of HIV today and the science behind U=U. Get tested for HIV and other STBBIs.
Wear a red ribbon
Make your own red ribbon and wear it leading up to and after World AIDS Day. Muluba will show you how!
Sexfluent.ca is a digital resource to learn about sexual health, mental health and harm reduction. Produced by CANFAR, Sexfluent is a trusted source for HIV 101.
You can order HIV self-test kits for free to your home. They’re a safe, accurate and private way to learn your status. If you test positive, you can get connected to care.
Share a message of support for people living with HIV and help us end HIV stigma in this generation.
Visit our campaign partners to learn more about the HIV/AIDS response in your area.
A word from our campaign partner, Gilead Sciences Canada.
“This marks our third year partnering with CANFAR on the national campaign, and we’re incredibly proud to support the many frontline organizations across Canada bringing attention to HIV and driving action.
Our commitment remains focused on the people most affected by this epidemic—ensuring that every individual has access to the care and support they need.
By staying true to this mission, we aim to help end the HIV epidemic for everyone, everywhere.”








































































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}